Why Do I Get to My Front Door and Am Bursting to Pee?


If you find yourself desperately rushing to the toilet the moment you put your key in the front door, you are not alone. This article explains exactly why this happens, what is going on inside your bladder and nervous system, and what you can do to break the cycle. Understanding the cause is the first step to regaining confidence and control.
Understanding the "Key in the Door" phenomenon and how to regain control
What Is "Latchkey Incontinence" or "Key in the Door Syndrome"?
This section explains the name behind the experience you may have been quietly putting up with for years, and why it is far more common than most people realise.
Latchkey incontinence, also known as key in the door syndrome, describes the sudden, overwhelming urge to urinate that strikes specifically when you arrive home. It is that all-too-familiar moment: the journey home was absolutely fine, but the second you reach your own front door, the urgency becomes almost unbearable.
This is not a coincidence. Latchkey incontinence is a well-documented conditioned response, meaning the body has been trained over time to associate a specific moment - arriving home - with the need to empty the bladder. The front door itself has become a trigger.
It is important to distinguish between the occasional need to rush to the toilet and a recurring pattern. Most people will experience urgency from time to time, especially if they are dehydrated or have been holding on for a long time. But if this happens every single time you come home, whether or not you actually need to go, that is a pattern worth paying attention to.
What is especially important to understand is how common this is, and how many women quietly dismiss it as normal. Many assume it is simply part of getting older, having had children, or just "how their bladder works". But latchkey incontinence is a recognised condition, and one that responds very well to the right support. You deserve to know that this is not something you just have to accept.
The science behind why it happens at the front door
The role of the brain and conditioned associations
To understand latchkey incontinence, it helps to understand what is happening in the brain, because this is far more a brain story than a bladder story.
The brain is remarkably good at forming associations between specific environments, actions, and physical responses. Every time you arrive home and rush straight to the toilet, you are reinforcing a powerful learning loop. Over time, your brain begins to connect the sensory experience of arriving home, the sound of your key turning, the feel of the door handle, (even the smell of your hallway), with the signal "time to urinate". The association becomes so strong that the brain starts sending urgency signals in anticipation, before any real physiological need exists.
This is essentially Pavlovian conditioning, the same process famously demonstrated in Ivan Pavlov's experiments with dogs salivating at the sound of a bell. Your front door has become your bell. The brain hears the "bell" and your bladder responds, not because it is full, but because the brain has learned to expect urination at that moment.
Crucially, anticipating reaching the toilet actually accelerates this urgency. As you approach your front door, the thought "I'll be able to go soon" intensifies the sensation. The closer you are to the perceived safety of your bathroom, the stronger the signal becomes. Many women find the urge is far worse at the door than it was during the entire journey home, and above is exactly why.
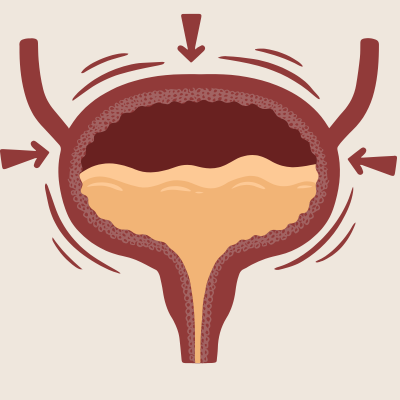
How the bladder and detrusor muscles respond
While the brain is sending the trigger signal, the bladder itself has a physical role to play in these urgency episodes.
The detrusor muscle is the muscle that surrounds the bladder wall and contracts to push urine out when you urinate. Under normal circumstances, it remains relaxed as the bladder fills and only contracts when you consciously choose to void. In overactive bladder syndrome, the detrusor becomes overactive, contracting prematurely in response to triggers, including conditioned ones like the front door.
What is important to understand is that when urgency strikes at the door, your bladder may not actually be full. The contraction is neurologically triggered rather than caused by a genuinely full bladder. The brain has sent a message, the detrusor has responded, and the sensation of desperate urgency follows, even when there is very little urine to pass.
Alongside the detrusor, your sphincter muscles and pelvic floor muscles play a crucial role in whether you are able to hold on. These muscles work together to maintain closure of the urethra and resist the involuntary detrusor contraction. When the muscles are strong and coordinated, you have a much better chance of suppressing the urge at the door. When they are weakened or poorly coordinated, which is very common, *and nothing to feel embarrassed about), the gap between urgency and leakage narrows.
Why the front door specifically acts as a trigger
You might wonder why it is always the front door, why not the car park, or the garden gate, or the street outside? The answer lies in the specificity of conditioned associations.
The front door brings together a unique cluster of sensory cues: the specific sound of your key, the physical sensation of turning it, the sight of your own home, the familiar smells of your hallway. These cues are deeply embedded as the final signal before bathroom access, and they fire together, creating an extraordinarily powerful trigger.
Interestingly, knowing the toilet is just metres away actually intensifies the urge rather than calming it. This is because proximity to the goal activates the brain's anticipatory response even more strongly. The sensation peaks not during the journey home, but precisely at the door.
This also explains why you do not typically experience the same urgency at the office, in a supermarket, or in other places where toilets are available. Those environments have not been repeatedly paired with bladder release in the same way. Your home bathroom is the specific endpoint your brain has learned to anticipate, and your front door is the final cue in that chain.
The connection to overactive bladder syndrome (OAB) and urge incontinence
Recognising OAB as the underlying condition
Latchkey incontinence rarely exists in isolation. In most cases, it is a symptom of a broader underlying condition that deserves proper attention and care.
Overactive bladder syndrome (OAB) is characterised by a cluster of symptoms: urgency (the sudden, compelling need to urinate), frequency (needing to urinate more than nine times in a day), nocturia (waking at night to urinate), and urge incontinence (leaking urine before reaching the toilet). You do not need to have all of these to be affected, urgency alone, including latchkey urgency, can indicate OAB.
OAB is not a structural problem with the bladder itself. It involves dysregulation of the nerve signals between the brain and the bladder, causing the detrusor muscle to contract at the wrong times. This is an important distinction because it means OAB is highly responsive to behavioural approaches and pelvic floor rehabilitation, it does not simply have to be managed with pads or avoidance.
It is also worth understanding the difference between urge incontinence and stress incontinence. Stress incontinence is leakage caused by physical pressure, coughing, sneezing and jumping. Urge incontinence is leakage driven by a sudden intense urge that the sphincter cannot hold back. Latchkey incontinence falls into the urge category. Distinguishing the two matters because the treatment approaches differ, and getting the right support for the right type makes a significant difference to outcomes.
Risk factors that increase susceptibility to OAB and conditioned urgency include hormonal changes around perimenopause and menopause, a history of pregnancy and childbirth, previous pelvic floor dysfunction, anxiety, and certain dietary habits. None of these are things to be ashamed of, they are simply factors that influence the bladder's sensitivity.
When urgency becomes leakage and accidents
For many women, latchkey urgency progresses beyond an uncomfortable rush, it becomes leakage, and sometimes a full bladder leak before they make it to the toilet.
The progression from urgency to leakage happens because the gap between the urgency signal and the sphincter's ability to hold, narrows over time. As the conditioned trigger becomes more ingrained and the overactive detrusor contractions become more forceful, the pelvic floor muscles struggle to hold back the contraction for long enough to reach the toilet. If this pattern is untreated, that gap continues to close.
The physical impact of leakage episodes is compounded by the emotional toll. Many women describe significant shame, embarrassment, and anxiety around the front door, planning arrivals to minimise risk, wearing pads every day, worrying about what would happen if they were delayed getting their key out. This is an exhausting way to live, and it is not something you should have to simply manage around.
Shame is one of the most significant barriers to seeking treatment. Many women live with these symptoms for years, sometimes decades, before reaching out for help. If you are experiencing leakage at the front door, that is a clear signal that your pelvic floor and bladder both need some targeted support. Reaching out is a courageous step, and the right practitioner will treat you with complete warmth and without judgement.
Practical Strategies to Stop the Urge at the Front Door
Urge Suppression Techniques to Use in the Moment
Urge suppression is a learnable skill, and it is one of the most empowering tools you can develop for managing latchkey incontinence. This section gives you practical techniques you can start using today.
The most important thing to understand is that urgency, although it feels uncontrollable, can be interrupted. The brain sent the signal AND the brain can also be redirected. The first technique to talk about is the squeeze and hold. When urgency strikes, firmly squeeze and lift your pelvic floor muscles. This creates a physical counter-pressure against the detrusor contraction and sends an inhibitory signal back to the bladder. Rather than rushing for the toilet, you stop, squeeze, and hold until the wave of urgency passes. It will pass.
Distraction is another highly effective tool. Mental arithmetic e.g. counting backwards from 101 in sevens (94, 87, 80 etc) redirects the brain's attention away from the bladder urgency signal. Focusing on a task that is a mental challenge for your brain, such as reciting the alphabet backwards or recalling family members birthdays can have the same effect. The urgency that feels all-consuming can be significantly reduced by redirecting brain activity.
Controlled, slow breathing calms the nervous system and reduces the intensity of urgency. Taking slow, deep breaths when the urge strikes lowers the physiological arousal that amplifies the sensation. Mindfulness techniques, simply observing the urgency without reacting to it, naming it as a sensation rather than an emergency, can be surprisingly powerful once practised.
The one thing I would advise against doing when urgency strikes is to rush to the toilet. Movement intensifies urgency, and rushing also focuses your entire attention on getting to the toilet and this amplifies the brain-bladder signal further. Standing still, breathing, and engaging your pelvic floor and holding your perineum to give extra support gives you the best chance of regaining control.
Breaking the Conditioned Association with the Front Door
Because latchkey incontinence is a learned response, the solution involves unlearning it. This is absolutely possible with the right approach and a little patience with yourself.
Deliberately changing your arrival-home routine is the starting point. If you have always rushed through the door and gone straight to the toilet, your brain needs new experiences to begin forming a different association. Start by pausing outside your front door before you enter. Use that moment to practise urge suppression. Squeeze, breathe, and hold your perineum, mental challenge until the wave passes. Then enter calmly, without going straight to the toilet.
This is where mindfulness becomes particularly useful. Many women find that anticipatory thoughts begin well before they reach the door like "I hope I make it," "I need to go as soon as I get in." These thoughts actively fuel the urgency. Learning to notice these thoughts without acting on them is part of retraining the brain's response.
Every time you successfully suppress the urge at the door rather than rushing to the toilet, you are weakening the conditioned association. The brain learns that the front door no longer needs to signal immediate bladder release. Over time, and it does take consistent repetition, the urgency at the door reduces and eventually resolves. Be proud of yourself for each small win along the way. Progress with this is absolutely something to celebrate.
Bladder Training as a Structured Approach
Bladder training is an evidence-based programme that works to recalibrate the brain-bladder relationship over time, and it is particularly effective for latchkey incontinence.
The principle is straightforward: you gradually extend the intervals between urinations, training the bladder to tolerate increasing amounts of urine and the brain to relearn what a genuinely full bladder feels like. Rather than responding to every urgency signal (many of which are false alarms) you begin to take back control over when and how often you empty your bladder.
A bladder diary is a really helpful tool at this stage. Recording when you drink, when you urinate, and when you experience urgency episodes (including front-door urgency) helps you identify your patterns, your most common triggers, and how your bladder behaves across a typical day. It also gives a baseline against which you can measure your progress and progress is something worth tracking and acknowledging when you are living with these symptoms daily.
Bladder training works best when it is combined with urge suppression techniques and professional guidance. A pelvic floor physiotherapist can help you build a personalised programme that works with your specific pattern of symptoms, your lifestyle, and your goals. It is not a one-size-fits-all approach, and you deserve a plan built around you.
Pelvic Floor Exercises and Physical Therapy
Strengthening the pelvic floor is a direct and effective physical intervention for latchkey incontinence and it is never too late to start.
Kegel exercises, the deliberate contraction and relaxation of the pelvic floor muscles, build the strength and endurance needed to resist involuntary detrusor contractions. A strong, well-coordinated pelvic floor provides the physical mechanism to hold on when urgency strikes at the door, buying you the time to apply urge suppression techniques and regain control.
However, technique matters enormously. Many women who have been doing Kegels for years are not performing them correctly and we know that incorrect technique can worsen symptoms rather than improve them. Bearing down, holding your breath, or tensing your buttocks instead of isolating the pelvic floor are all common errors that a professional assessment can identify and correct.
Pelvic floor physical therapy goes beyond Kegel exercises. A specialist pelvic floor physiotherapist can assess the tone, strength, and coordination of your pelvic floor muscles, identify whether over-activity or weakness is playing a greater role in your symptoms, and design a genuinely personalised programme targeting your specific urgency triggers. This is evidence-based, specialised care and it is exactly what you deserve.
Lifestyle Changes and Long-Term Management
Habits and Behaviours That Worsen Front-Door Urgency
Some of the habits we form around bladder urgency, with the best of intentions, actually make the problem worse over time. Understanding these patterns is an important part of long-term management.
The most reinforcing habit of all is rushing to the toilet the moment you arrive home. Every time you do this, you strengthen the conditioned trigger. The brain learns - front door equals immediate bladder release. Breaking this habit gradually and with support is central to recovery.
Caffeine and alcohol are two of the most well-known bladder irritants, increasing both frequency and urgency by irritating the bladder wall and increasing urine production. If you drink several coffees a day or regularly consume alcohol, reducing intake can make a noticeable difference to bladder sensitivity. Staying well hydrated with water, however, is important concentrated urine irritates the bladder further.
Anxiety and stress significantly amplify the brain-bladder urgency response. The nervous system is already primed and reactive in a state of stress, which lowers the threshold for urgency triggers. If you are going through a particularly stressful period, you may notice your front-door urgency is worse.
"Just in case" peeing is going to the toilet before you leave the house even when you do not need to. It is a habit that can reduce bladder capacity over time. The bladder learns to expect to be emptied at lower and lower volumes, and urgency at smaller volumes increases. It feels like a sensible precaution, but it reinforces rather than resolves the problem.
Stress Reduction and Mindfulness as Supportive Tools
The relationship between the nervous system and the bladder is closer than most people realise and managing stress is a genuinely meaningful part of addressing latchkey incontinence.
Chronic stress keeps the nervous system in a heightened state of alertness, which means the threshold for urgency triggers (including the front door) is lowered. A nervous system under chronic pressure is a more reactive nervous system, and the bladder responds to that reactivity.
Mindfulness-based approaches are particularly useful for latchkey incontinence because so much of the response is driven by anticipatory thinking. Learning to observe the sensation of urgency without immediately reacting to it. Noticing it, naming it, and letting it pass without rushing is a skill that can be practised and developed. It does not require hours of meditation and even a few minutes of focused breathing daily builds meaningful nervous system regulation over time.
Stress reduction practices. Whether that is regular movement you enjoy, time in nature, quality sleep, or dedicated relaxation, support the effectiveness of bladder training and urge suppression. They create a physiological environment in which retraining is easier. Addressing the psychological anticipation of the front-door trigger is just as important as the physical pelvic floor work, they work together, not in isolation.
When to Seek Professional Treatment Options
Self-management strategies are powerful and genuinely effective for many women but they are most effective when combined with professional support, and there are clear signs that you should not try to manage this alone.
If you have been experiencing front-door urgency for more than a few weeks, if urge suppression techniques are not providing adequate relief, if you are experiencing leakage or accidents, or if your symptoms are affecting your confidence, your social life, or your daily activities, those are all clear signals to seek a professional assessment. You do not need to wait until things are significantly worse. Early intervention is always better than waiting.
Treatment options for OAB and latchkey incontinence span a range, depending on the severity and underlying factors involved. Pelvic floor physical therapy and bladder training programmes are first-line, evidence-based approaches that address the root causes directly. For some women, medication may be appropriate alongside behavioural approaches, and a healthcare provider can assess whether this is right for your situation. In cases where conservative approaches have not produced sufficient results, further medical options exist. However the vast majority of women see meaningful improvement with behavioural therapy and pelvic floor rehabilitation.
A specialist will assess your symptoms, take a full history, and rule out other causes such as urinary tract infections, prolapse, or post-menopausal changes that may be contributing. This is not an embarrassing conversation to have, it is a clinical one, and a good practitioner will put you completely at ease.
Latchkey incontinence is a recognised, treatable condition. It is not something you imagined, it is not something you simply have to put up with, and it is not a reflection of weakness. Please reach out without embarrassment. You deserve to feel confident and in control, whatever door you are walking through.
Key Takeaways
Latchkey incontinence is the overwhelming urge to pee the moment you reach your front door. It is a well-documented conditioned response rooted in the brain-bladder connection, not a sign that something is irreparably wrong with your body. The front door has become a learned trigger, training the detrusor muscle to contract prematurely through repeated association with bladder release. The urgency you feel is often not a reflection of genuine bladder fullness, but a neurologically-driven response that can be interrupted, retrained, and resolved. Practical strategies including urge suppression techniques, bladder training, and pelvic floor rehabilitation are highly effective, and combining these with professional guidance gives the best outcomes. If this experience is affecting your life, please know that you are not alone, this is entirely treatable, and you deserve the support to reclaim your confidence and freedom.